Diabetic retinopathy care in Suwanee, GA — early detection, expert monitoring
★★★★★
5.0 from 275+ Google Reviews
Castle Connolly Top Doctor
American Board Certified
5 Million Educational Views
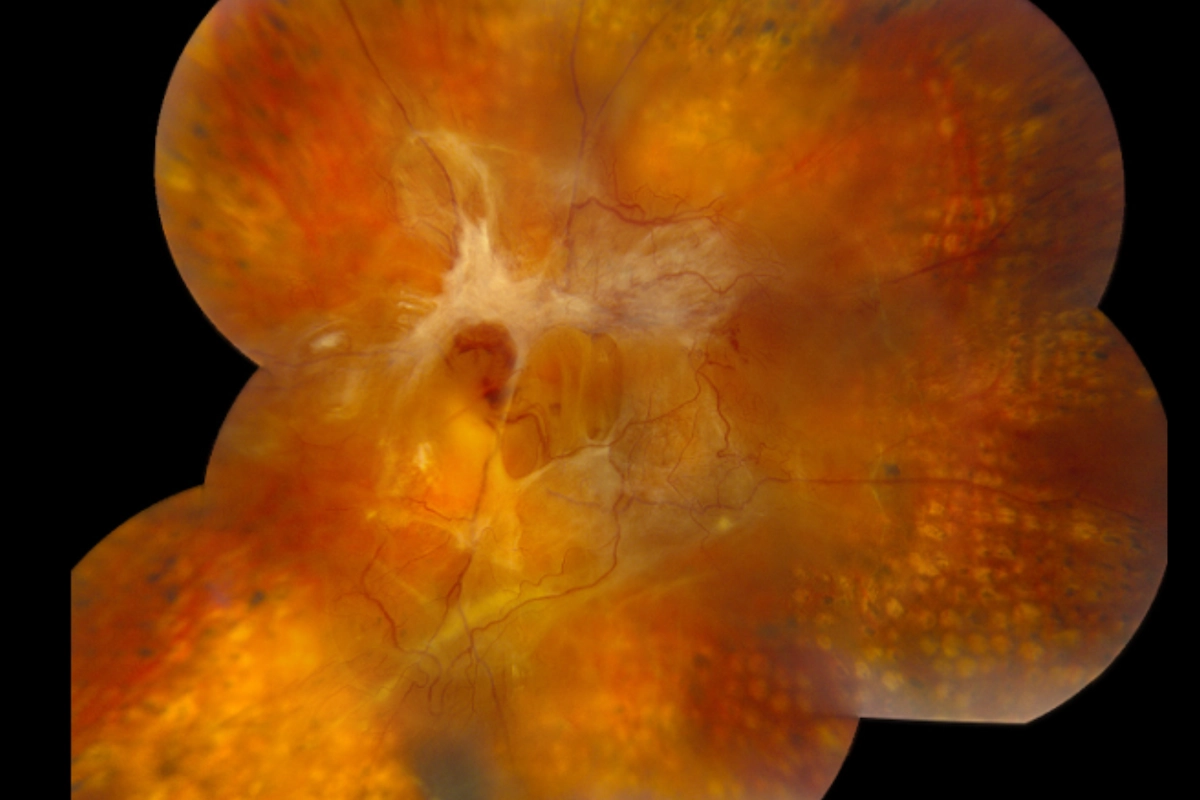
Diabetic retinopathy is the leading cause of preventable blindness in working-age adults in the United States. At Stratus Eye, Dr. Jeffrey Tran brings experience managing some of the most advanced cases in the country — and the same standard of care to every diabetic patient who walks through our door.